
Royal Dental College
E-ISSN: Coming Soon
E-ISSN: Coming Soon
Correlation of Dermatoglyphic Patterns with the Prevalence of Dental Caries in School Children
Full Html
INTRODUCTION
Dermatoglyphics originates from the Greek terms 'derma,' which means skin, and 'glyphic,' which refers to carvings. It pertains to the scientific examination of the epidermal ridge patterns found on fingers, palms, toes, and soles. The concept was first introduced by Harold Cummins and Midlo in 1926. These ridge patterns are genetically predetermined, unique to each person, and do not change throughout an individual's life.[1] This consistency and individuality render fingerprints an essential tool for identification. Fingerprint analysis, known as dactylography, has been a fundamental aspect of forensic science for more than 150 years. It is extensively utilized for security, authentication, and personal identification purposes worldwide. Additionally, dermatoglyphics has demonstrated its value in various disciplines, including biology, medicine, genetics, and evolutionary studies, owing to its capacity to offer insights into human development and heredity.[2,3] Dental caries is a complex disease influenced by genetic, environmental, microbial, and behavioral factors.[4] Recently, dermatoglyphics has attracted interest as a non-invasive and cost-effective screening method for identifying individuals at risk for specific diseases. The rationale for investigating dermatoglyphics in connection with dental caries stems from the shared ectodermal origin of dental enamel and epidermal ridges. Both structures develop during the same phase of intrauterine life, indicating that genetic anomalies affecting one may also impact the other. Nevertheless, the evidence regarding its link to dental caries remains inconsistent. Consequently, the current study was conducted to assess the relationship between dermatoglyphic patterns and dental caries in school children.
MATERIALS AND METHODS
A cross-sectional study was carried out involving 203 school children (100 males and 103 females) aged between 13 and 15 years. Participants were randomly chosen from various schools after securing the necessary permissions. Ethical approval was granted by the Institutional Ethical Committee, and the study adhered to both local and international ethical guidelines. Written informed consent was acquired from parents or guardians, while assent was obtained from the children themselves. The study included children aged 13 to 15 years who were cooperative and willing to participate, had fully erupted teeth, and were
otherwise healthy. Exclusions were made for children with systemic diseases, developmental anomalies, or finger deformities that could hinder fingerprint recording, as well as those undergoing orthodontic treatment.
The right thumb of each participant was cleaned and dried. Fingerprint impressions were obtained using an ink pad and transferred onto white chart paper. The prints were examined using a magnifying lens and classified into loop, whorl, and arch patterns according to standard dermatoglyphic classification. Dental caries experience was recorded using the Decayed, Missing, and Filled Teeth (DMFT) index following World Health Organization (WHO) criteria. All examinations were performed under adequate illumination using mouth mirrors and explorers. Data were entered into a spreadsheet and analysed using appropriate statistical software. The Chi-square test was used to assess associations between fingerprint patterns, gender, and dental caries experience. A p-value of <0.05 was considered statistically significant.
RESULTS
This cross-sectional prospective study was conducted to compare the finger print pattern with and the association of finger print with gender and dental caries. 203 school children in the age of 13-15years participated in the present study of which 100 were males and 103 females. Among the pattern of finger print loop pattern was the most prevalent pattern in both genders with slightly higher count in males 6 and 57 females followed by second most common pattern, the whorl pattern 28 males and 29 females. The least common type of finger print pattern was arch pattern found frequently in 19 females and 9 males. (Chart 1)
.jpg)
Chart 1 Bar graph distribution of dermatoglyphic among males and females
The relationship between gender and dermatoglyphic patterns was assessed through the chi-square test of independence. The distribution of loop, whorl, and arch patterns was analyzed among both males and females. The results of the chi-square analysis indicated that there was no statistically significant association between gender and the distribution of dermatoglyphic patterns, as the p value exceeded 0.05. While minor variations were noted, including a slightly elevated frequency of loop patterns in males and arch patterns in females, these differences did not achieve statistical significance. (Table 1)
| Dermatoglyphics patterns | Males n(%) | Females N(%) |
Loop pattern | 61 (62.9%) | 57 (54.8%) |
Whorl pattern | 28 (28.9%) | 29 (27.9%) |
Arch pattern | 9 (9.2%) | 19 (18.3%) |
Total | 98 (100%) | 105 (100%) |
X2=3.49 df=2 p=0.175 (not significant) | ||
Table 1 showing correlation of finger print pattern with gender
The distribution of dermatoglyphic patterns concerning dental caries status is illustrated in Table 2. In children without dental caries, the loop pattern was the most common (72), followed by the whorl pattern (36) and the arch pattern (15). A similar pattern was noted in children with dental caries, where the loop pattern was still the most prevalent (46), followed by the whorl (21) and arch patterns (13). In summary, loop fingerprints made up the majority in both caries-free and caries-affected groups, while arch patterns were the least frequent. Although the total counts of all fingerprint patterns were greater in the caries-free group compared to the caries-present group, the relative distribution pattern was consistent across both groups. This indicates a predominance of loop patterns regardless of dental caries status. (Chart 2)
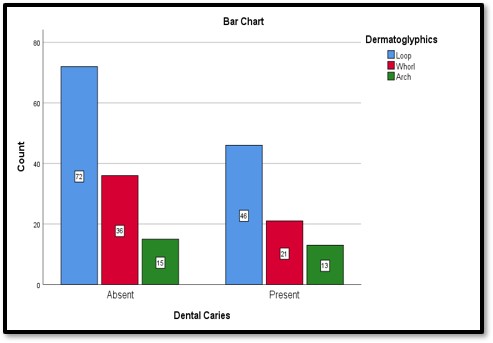
Chart 2 Bar graph showing distribution of dermatoglyphic with or without dental caries
A chi-square test was conducted to evaluate the relationship between dermatoglyphic patterns (loop, whorl, arch) and the status of dental caries (present/absent). In the group of caries-free children, the distribution of patterns was 58.5% for loops, 29.3% for whorls, and 12.2% for arches. Conversely, in children with dental caries, the respective proportions were 57.5% for loops, 26.3% for whorls, and 16.3% for arches. The results of the chi-square analysis indicated that there was no statistically significant association between the distribution of fingerprint patterns and the occurrence of dental caries (p > 0.05). (Table 2)
Finger print pattern | Without dental caries | With dental caries | Total |
Loop pattern | 72 (58.5%) | 46 (57.5%) | 118 (58.1%) |
Whorl pattern | 36 (29.3%) | 21 (26.3%) | 57 (28.1%) |
Arch pattern | 15 (12.2%) | 13 (16.3%) | 28 (13.8%) |
Total | 123 (100%) | 80 (100%) | 203 (100%) |
X2=0.66 df=2 p>0.05 (not significant) | |||
Table 2 showing correlation of finger print pattern with and without dental caries
Statistical analysis conducted with the Chi-square test indicated that there was no significant correlation between fingerprint patterns and gender (p > 0.05). Likewise, no statistically significant relationship was found between fingerprint patterns and dental caries experience, as assessed by the DMFT index (p > 0.05).
DISCUSSION
Fingerprints, which are the unique patterns formed by the tiny ridges on fingertips, are extremely individualized and play a vital role in forensic identification, particularly in criminal cases and the identification of victims in mass disasters.[5] Identifying individuals, whether they are alive or deceased, is fundamental to forensic science. This identification process is heavily dependent on the examination of distinct physical and mental characteristics, which are essential tools in forensic investigations. Among the different types of trace evidence, fingerprints have become one of the most dependable and commonly utilized methods for personal identification. The scientific discipline that studies fingerprints, referred to as dermatoglyphics, concentrates on the naturally occurring epidermal ridges present on fingers, palms, and soles, along with the flexion creases and secondary folds.
In ancient India, the study of edge configuration was referred to as 'Samudra Shastra'. The designs of the epidermal edges were categorized into 'Chakra, Shankya, and Padma', which correspond to the Whorl, Loop, and Arch patterns. The earliest examination of fingerprint patterns in India was conducted by William Herschel in 1880.[6] The term 'dermatoglyphics' was coined by anatomist Harold Cummins in 1926, who found that the patterns of these ridges are shaped by both genetic influences and environmental factors during fetal development.[7] These projections ultimately create the distinct patterns of papillary ridges, which are fully formed between the 11th and 24th weeks of gestation.[8] Dental caries is the most common disease among humans and is influenced by multiple factors. It has been noted that the pattern of caries is similar across several generations of family members; thus, inheritance is suggested.[9]
The current study assessed the relationship between dermatoglyphic patterns and dental caries in school children aged 13 to 15 years. There was a slight majority of females compared to males in this study. The analysis of dermatoglyphics revealed a significant prevalence of the loop pattern in both genders, indicating that loops are the most common type of fingerprint pattern regardless of sex. Although males exhibited a slightly higher occurrence of loop patterns than females, the difference was negligible. Whorl patterns were found at similar rates in both sexes, indicating no significant gender-based differences. Arch patterns were the least common overall; however, a somewhat higher frequency was observed among females than males. This suggests that the distribution of dermatoglyphic patterns is not influenced by gender in the studied population.[10,11] These results imply that while the overall distribution of dermatoglyphics is alike between genders, there are minor differences, especially in the frequency of arch patterns.
The distribution of dermatoglyphic patterns was similar in both groups, suggesting that while loop patterns were the most common, there was no significant correlation between fingerprint pattern type and dental caries status in the study population. Interpretation: No statistically significant link was found between dermatoglyphic patterns and dental caries status. The distribution of loop, whorl, and arch patterns was similar in children with and without dental caries. Our findings align with those reported by Ahmed et al (2017).[12] The lack of a significant relationship between fingerprint patterns and gender noted in this study is consistent with several earlier reports.[13-15]
However, earlier research conducted by Chinmaya et al. in 2016 and Pooja et al. in 2022 indicated that the whorl pattern of fingerprints is linked to a higher DMFT score, while the loop pattern correlates with a lower DMFT index.[6,16] Additionally, the absence of a relationship between dermatoglyphic patterns and dental caries implies that fingerprint patterns alone may not serve as reliable indicators of caries susceptibility. Discrepancies found in the literature could stem from differences in study design, population characteristics, age groups, sample sizes, and methods used for caries assessment. Future research involving larger sample sizes, longitudinal designs, and the inclusion of genetic and environmental factors may yield more definitive evidence concerning the role of dermatoglyphics in predicting the risk of dental caries. Therefore, documenting the dermatoglyphic patterns of children during their initial dental visit at a young age could
be beneficial in determining whether a child is part of a high-risk or low-risk group, thus assisting in the development of an effective preventive and treatment strategy.
CONCLUSION
Based on the constraints of the current study, it can be inferred that the loop pattern is the most prevalent dermatoglyphic pattern found in school children aged 13 to 15 years. There was no significant correlation identified between fingerprint patterns and either gender or the experience of dental caries. Therefore, dermatoglyphics may have restricted usefulness as an independent screening method for assessing the risk of dental caries.
References
1. Cummins H, Midlo C: Palmar and plantar epidermal ridge configuration (dermatoglyphics) in Europeans and Americans. American J Biological Anthropology. 1926;9:471-502.
2.Krishan Vij: Textbook of Forensic Medicine and Toxicology Principles & Practice 6e. Krishan Vij (ed): Elsevier India Pvt. Limited, India; 2014.
3.Kanchan T, Chattopadhyay S: Distribution of fingerprint patterns among medical students. J Indian Acad Forensic Med. 2006;28:65-8.
4.Cogulu D, Saglam C. Genetics aspects of dental caries. Frontiers of Dental Medicine 2022;3:1-5. doi.org/10.3389/fdmed.2022.1060177.
5.Kucken M, Newell AC: Fingerprint formation. J Theor Biol. 2005;235:71-83.
6.Monpara PC, Odedra SP, Shah KH, Dodia VS, Pillai JP, Yadav S. The relationship between arch, loop and whorl fingerprint patterns with dental caries: A cross-sectional, descriptive institution-based study. Journal of Oral Medicine, Oral Surgery, Oral Pathology and Oral Radiology. 2022;8(2):69-75. doi.org/10.18231/j.jooo.2022.014.
7.Bhat GM, Mukhdoomi MA, Shah BA, Ittoo MS. Dermatoglyphics: in health and disease - a review. International Journal of Research in Medical Sciences. Int J Res Med Sci. 2014 Feb;2(1):31-37.
8. Hamilton WJ, Boyd DJ, Mossman HW: Hamilton, Boyd & Mossman's Human Embryology Prenatal Development of Form and Function. Fourth Edition. Hamilton WJ, Mossman HW (ed): The Williams & Wilkins Co., Baltimore, USA; 1972.
9.Liu C, Lin J, Ostrburg J, Nicol J. Finger printcomparison II: Similarity of fingerprints. J Forensic Sci. 1982;27(2):290-304.
10.Chopra M. The study of finger print patterns among male and female. Indian Journal of Forensic Medicine and Toxicology 2020;14(4):408-413.
11. Ranjan SK, Kumari P, Singh NK, Kumar A, Kumar Sanjeev. Relation of primary fingerprint patterns with gender and blood groups: A dermatoglyphic study from a tertiary care Institute in Bihar. European Journal of Cardiovascular Medicine. 2025;15(3):293-299.
12. Ahmed SA, Hanan ES, Marwa MF. Forensic dissection of lip print as an investigative tool in a mixed Egyptian population. Alexandria Journal of Medicine. 2018;54:235-239. https://doi.org/10.1016/j.ajme.2017.08.002.
13. Patil A, Malik A, Shirole T. Fingerprint patterns in relation to gender and blood groups - A study in Navi Mumbai. Indian Journal of Forensic and Community Medicine 2017;4(3):204-208.
14. Eboh DEO. Fingerprint patterns in relation to gender and blood group among students of Delta State University, Abraka, Nigeria. Journal of Experimental and Clinical Anatomy 2013;12 (2):81-86.
15. Odokuma EI, Igbigbi PS, Emundianughe TS. A study of thumb print patterns and ABO Blood group distribution. J Exp Clin Anat 2008; 7(1): 22-26.
16. Chinmaya B, Smitha B, Tandon S, Khurana C. Dermatoglyphics: An indicator of dental caries in humans. J Indian Assc Public Health Dent. 2016;14(3):272-5.
